- Published on
Collaborative Healthcare with Technology
- Authors
- Name
- Ally Salim Jr
- @3210jr




Introduction
Healthcare is fragmented, not equitable, expensive, and very hard to scale. That said, governments and other organizations are working very hard to change the face of healthcare and its delivery, even with the massive setbacks from the COVID-19 pandemic. Among the many wins over the past few decades, there has been a global increase in life expectancy [Ref], decrease in malaria moralities[Ref] and under 5 mortality[Ref], as well as the eradication of diseases [Ref].
Despite those leaps of progress, we still have a long way to go as the challenges seem to be evolving faster than the solutions can [AMR, super bugs, covid-19, climate change + spillovers]. Luckily for us, technology can grow and develop just as fast, empower novel solutions, and fast track the trial and error processes to filter out sub-par solutions. In this article we will look at one dimension of the multidimensional problems in healthcare - Health Equity - and explore how technology can be leveraged for global health improvement.
Health Equity
We achieve health equity when everyone, everywhere, is able to attain their full health potential and no one is “disadvantaged from achieving this potential because of social position or other socially determined circumstances.”[Ref].
“Health equity is defined as the absence of unfair and avoidable or remediable differences in health among population groups defined socially, economically, demographically or geographically”. - WHO
A key ingredient of Health Equity is ensuring that everyone has access to high quality care services and decisions through qualified and experienced physicians and specialists. In overly simplistic terms, this means increasing the number of doctors and specialists to a suitable physician-patient ratio (PPR) so that there are enough highly-trained care providers to meet demand. According to the WHO, this means achieving a recommended minimum ratio of 4.5 physicians for every 1,000 population (4.5:1,000). Currently, the African continent averages 1.3 physicians per 1,000 population [Ref] - well below the minimum ratio for quality care.
Its easy to see that closing this gap is not easy to do. Humans are notoriously difficult to scale. Training a physician could take close to a decade and training a specialist takes even longer, not accounting for the (important) years needed to get field experience treating patients and encountering new situations.
Diseases do not read books, always trust your clinical acumen. [Ref]
The narrative gets even worse when considering specialists such as dermatologists, pediatricians, pulmonologists, cardiologists, and radiologists. These specialists can be found in developed cities and towns where the compensation rightfully matches their skills. Unfortunately, this leaves a majority of the continent (rural), severely underserved.
The unequal distribution of health specialists, in addition to the low numbers of them to begin with, results in the inequity of access to quality health decisions. Patients in rural areas are often misdiagnosed[Ref], poorly treated, and often given treatments like antibiotics without regard for downstream effects[Ref].
It is important to note that this is (at least) partially responsible for the high mortality and morbidity rates in Africa. Another side effect of this unequal distribution of knowledge and skills is how it affects the quality of prevalence data collected when the data collectors have high misdiagnoses rates.
Technology for Improved Health Decisions
For a few decades now, technology has been affecting every aspect of our lives and healthcare is no different - from the use of EHRs for patient history management to the use of telemedicine to reach specialists thousands of kilometres away.
The technologies of interest in this article are Artificial Intelligence, Machine Learning and Federated/Collaborative Learning.
Artificial Intelligence: Intelligence exhibited by computers and machines. This is a fast growing field of research at the intersection of many domains with computer science and mathematics.
Machine Learning: Similar to how humans learn through examples, extrapolation, analogies, and educated guesses with trial & error, machine learning refers to the process of computers learning to solve a given problem just by looking at the examples provided (historical data) and taking the learned skills to be applied to new situations.
Federated Learning: Federated learning is a machine learning technique that trains an algorithm across multiple decentralized edge devices or servers holding local data samples, without exchanging them [Ref].
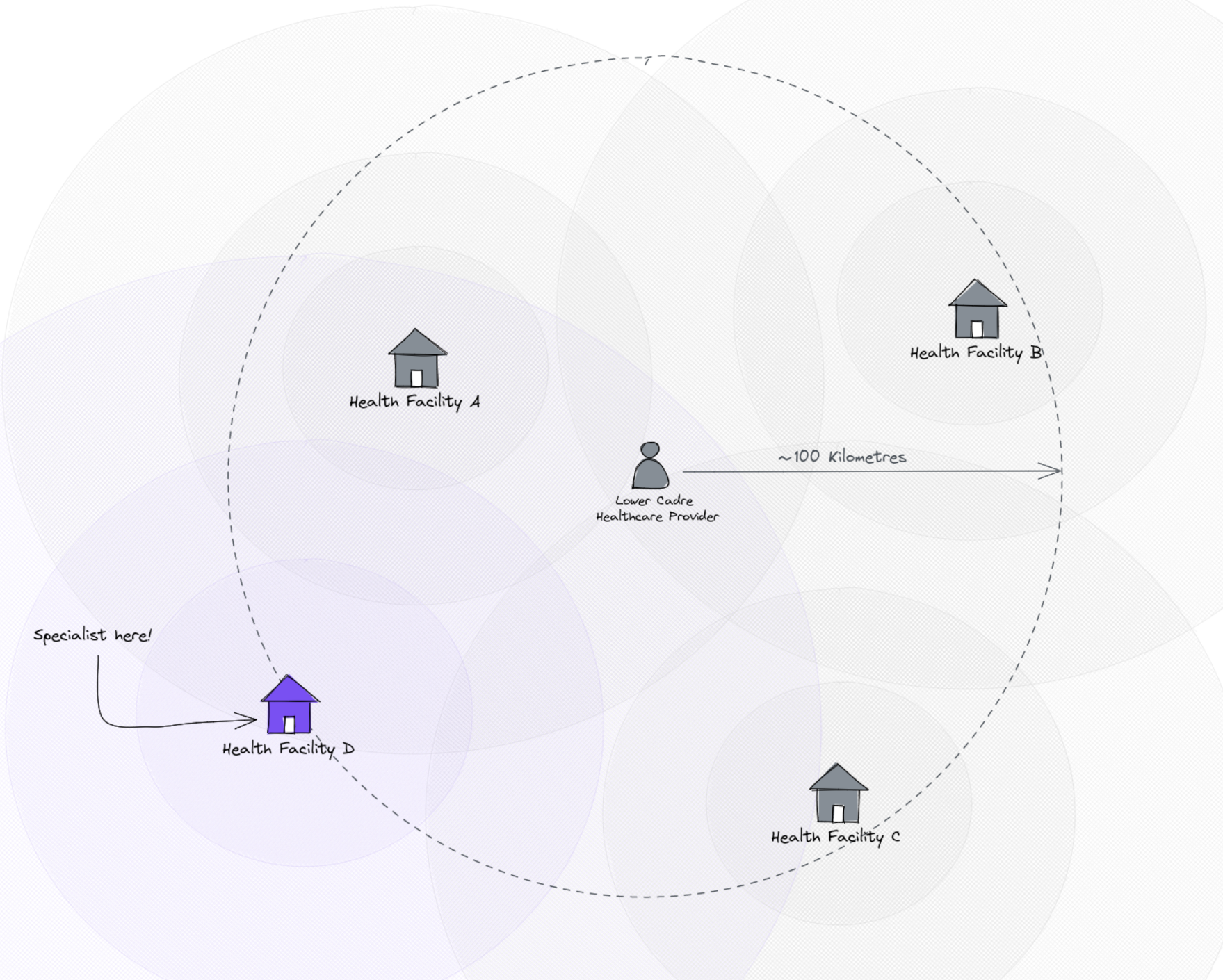
Simple Scenario Let's consider a community healthcare worker/clinical officer in a rural area of East Africa. We will call her Rose. Despite Rose's constant hard work and passion, she has received minimal training and her diagnostic abilities are poor compared to the specialists she one day hopes to become.
Within a 100 kilometre radius of Rose's jurisdiction, there are 4 hospitals with medical testing equipment, and of those 4, only one has a very experienced pediatrician.
Now that the scene has been set, let's explore how we can leverage advances in technology to increase the availability of quality health decisions.
Symptom Assessment, the healthcare provider: There is an abundance of engineers and health professionals worldwide working on Artificial Intelligence for symptom assessment, including the WHO/ITU Focus group on the subject[Ref].
These algorithms can be loaded onto a low cost smartphone of the care provider (availability of smartphones in rural areas is another problem entirely), and can be used offline to help assess the symptoms of the patient.
For simplicity, we will assume the disease identification algorithm is simply the product of likelihood of a given condition and the prevalence of that condition:
which, for Malaria, roughly translates to:
The likelihood function of a given condition is the main algorithm for identifying the underlying illness, whether its using Machine Learning or not.
Collaborative Care, standing on the shoulders of giants: The epidemiology and prevalence of disease presents itself in complex and very convoluted patterns. However, the prevalence of a condition can make an almost impossible diagnosis in one area, the best differential in another area.
Our community healthcare provider's technology, connected to the same technology used by the other 3 hospitals with testing equipment and the one with a specialist, can have access to both their improved decision support models (P(B | A)) and disease prevalence information (P(A)).

This is powerful for the poorly trained community healthcare worker, and this can scale almost infinitely.
The flow of knowledge, through the prevalence and likelihood models, is not limited to from the top (specialists) to the bottom (community care providers) - it can also be from the bottom to the top. Take for example the case of the skin condition scabies: most scabies cases are easily identified at the community level and do not make it to the higher levels of care, often for years.
The proposed solutions are not without their challenges, mainly a lack of reliable infrastructure, but the benefits and opportunities created far outweigh the costs.
Using Federated/Collaborative Learning approaches, we can leverage patient data within connected facilities in a privacy preserving ways that require no data to be transmitted from the host facility. Only all or some aspects of the models are shared with other members of the network.
A healthcare provider with 6 months of basic training can now assess patients with specialist algorithms that are supported by prevalence information from all other connected providers. This is a pretty good start.
Simplified Demo
Adjust the distances (Kms) between the healthcare provider and each facility as well as the condition prevalences to see how her decisions can be affected just by leveraging the skills of others.
Provider
Edit Configuration
Community Healthcare Worker
Leveraging the results of surrounding providersWhat we are doing at Elsa Health
At Elsa Health, we build AI technologies for decision support in rural and low resource areas of Africa. In our work, our algorithms benefit heavily from the shared and distributed architecture for sharing models and priors.
We use these solutions in:
- HIV: Medication adherence prediction, symptom assessment for HIV + patients, and tracking lost to follow up patients (LTFU).
- Pediatrics: Symptom assessment for children under 14 years.
- Anti-microbial Stewardship: Working with stakeholders to keep track of resistant pathogens (bacterial, enteric and fungal).
Reach out to us
To learn more about our work, or if you are interested in working together, please reach out to us through our website, or follow us on social media!
To contact us directly visit our site: elsa.health/contact